
ALGORITHM
Definitive care in 4 minutes for anaphylaxis.
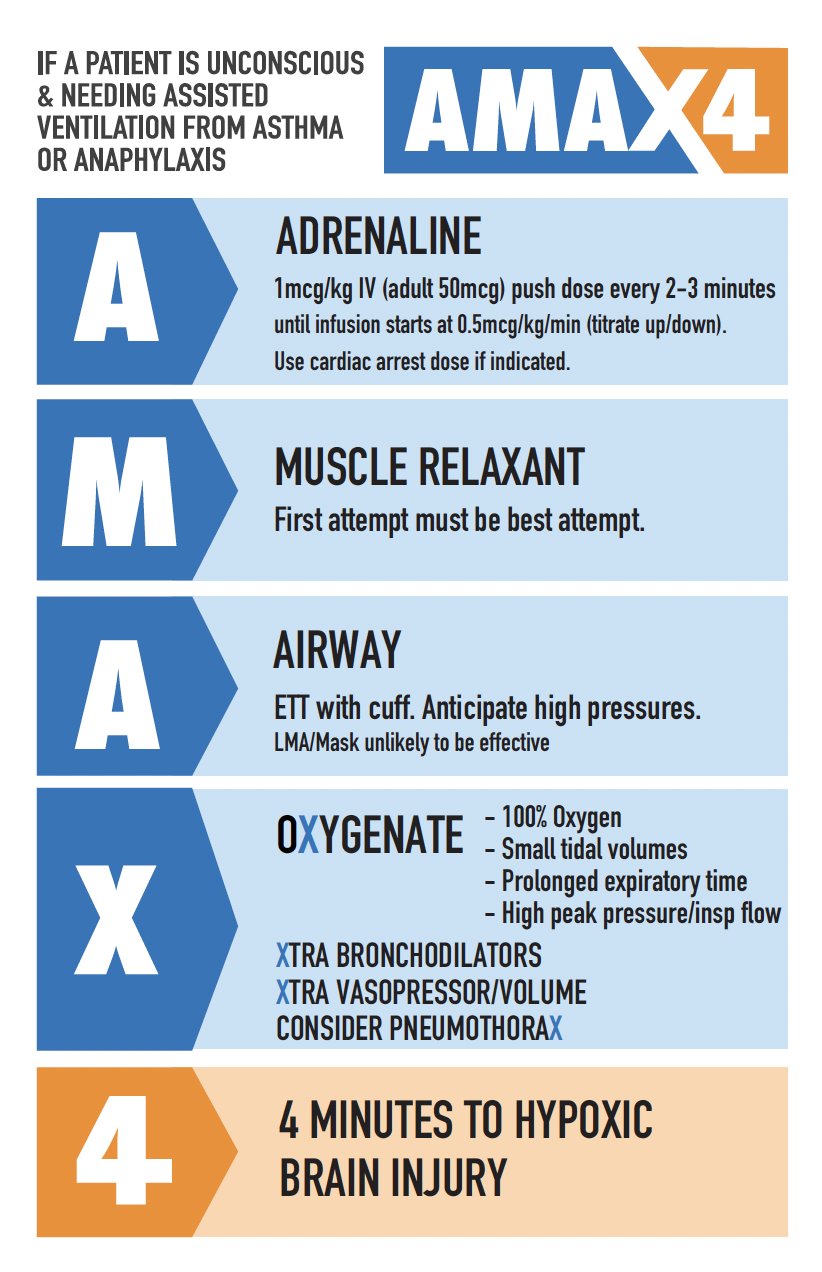
Why the algorithm?
The time to hypoxic brain injury is extremely short and cannot be extended by CPR in hypoxic arrest without oxygenation.
Food allergies are the most common triggers for young people presenting to an Emergency Department (ED). Almost all people who die from food anaphylaxis do so due to respiratory arrest from bronchospasm. Bronchospasm also occurs in drug and venom allergy and causes death. This algorithm also works in these cases.
The following observations led to the development of the algorithm:
Patients who are not breathing effectively or are unconscious requiring BVM support have decompensated from hypoxia and carbon dioxide accumulation.
Airway pressures required to oxygenate are high in bronchospasm — too high for anything other than an ETT. BVM and LMA are unsuitable. BVM is always the first device for oxygenation but an ETT should follow immediately as per ASCIA and ANZCOR guidelines.
The first attempt must be the best attempt with videolaryngoscopy. 40% of food allergy deaths have some airway swelling but the vast majority could be intubated without a surgical airway. A surgical airway should occur in the rare situation where intubation is not possible (>8 years old).
Aspiration risk is high (40% of food deaths aspirate), and the consequences can be catastrophic; and
Intubation is inevitable - why not do it before hypoxic brain injury?
See the Evidence page for further information
How does the algorithm help clinicians?
By understanding:
The pros and cons of medical devices used for oxygenation
The pharmacokinetics and risks/benefits of IM vs IV adrenaline in decompensating patients.
Risk of obstructive hyperinflation
Risk of pneumothorax and
How to perform difficult ventilation in the face of high pressures and an obstructive pattern using a laerdal bag post-intubation.
Who should use this algorithm?
This algorithm applies to all clinicians who are capable of endotracheal intubation or are part of an intubating team including paramedics, doctors, and nurses.
Non-intubating clinicians need to understand that it is unknown how long bag valve mask ventilation can oxygenate someone with critical asthma/anaphylaxis or severe airway obstruction before it fails.
The most senior person needs to devote every effort to deliver oxygen — a two-person BVM technique may help.
Fulminant bronchospasm does not usually occur in pre-school aged children and this algorithm should not be used for this group.